Italian Journal of Intellective Impairment 10 (2): 143-9 (1997)
Via A. Rabbeno, 3
42100 Reggio Emilia, Italy
+39 0522 320 716
Mobile +39 348 5145 520
URL: http://www.stress-cocchi.net
Riverbend DS Assocation Home Page »
» Drug Therapy » Easiness to URTIEasiness to Upper Respiratory Tract Infections: An Investigation on 510 Down's Syndrome Persons |
Author article list |
|
Renato Cocchi M.D., Ph.D. (Sociology) Italian Journal of Intellective Impairment 10 (2): 143-9 (1997) |
Reprinted with the permission of Renato Cocchi Via A. Rabbeno, 3 42100 Reggio Emilia, Italy +39 0522 320 716 Mobile +39 348 5145 520 URL: http://www.stress-cocchi.net |
Key words: Down's syndrome; Upper Respiratory Tract Infections; Easiness; Age.
In previous research published more than 16 years ago and devoted to easiness to Upper Respiratory Tract Infections (URTI) in depressed children, I noticed its lowering or disappearance following drug treatment of glutamine, pyridoxine and a low dose benzodiazepine. There I reported my first Down's syndrome patient, a 9 years old child with URTI easiness (Cocchi, 1981, patient no. 15).
The therapy aimed to treat this specific symptom, but the results on other symptoms were so unexpected to encourage treating other Downs, even when this symptom was not present, as I saw later (Cocchi, 1990).
This easiness was the starting point for applying to Downs a drug therapy well working in depressed children. Such a symptom had always a careful checking during 1st consultations of 510 trisomic people. Epidemiological and clinical-therapeutical information so collected were partly processed, as the aim of previous research (Cocchi, 1987; Cocchi and Bonaduce, 1988; Cocchi, 1990).
I came back on this topic with a larger casuistry and a more differentiate point of view.
Materials and methods
This investigation used the clinical cards referring to a non selected consecutive series of home reared and home living Downs as seen in outpatients clinic by the present author between January 1979 and April 1997.
During their 1st consultation all these subjects had their easiness to URTI evaluated and recorded by severity, along with other signs and symptoms.
This easiness was appraised with reference to the past 12 months (or, in children aged less than one year, with reference to past months) by recording according to a severity scale as follows:
(0) = as in a healthy child;
(1) = nasal catarrh usually present;
(2) = 1 + susceptibility to cough and cold with a few feverish episodes;
(3) = 1 + 2 + easiness to tonsillitis, pharyngitis, bronchitis with moderate fever and limited need of antibiotics (up to four regimens per year);
(4) = 1 + 2 + 3 + high temperatures, occasional otitis and bronchial pneumonia, and frequent use of antibiotics (more than four regimens per year).
From all the records so pointed out those pertaining to autistic or PDD DS Ss were discarded because we saw that this second heavier pathology can modify the URTI easiness (Cocchi and Bonaduce, 1988).
From the remaining records I collected: sex; chromosomal diagnosis; age at 1st consultation; easiness to URTI according to the severity scale.
I processed data by age intervals statistics and I applied Chi Square Test, when suitable.
Results
Only 510 records out of 548 fitted the criteria for this research. Data referring to subjects checked have their reports in tables 1-12, by sharing them according to two years age intervals, as for URTI easiness.
Graphs 1-2 show time course of this easiness and its severity according to age.
| No. of Ss | 510 | 100.00% |
| males | 292 | 57.25% |
| females | 218 | 42.57% |
| M/F ratio | 133.94/100 | |
| Chromosomal diagnosis | ||
| standard trisomy 21 | 461 | 90.39% |
| mosaicisms | 16 | 3.14% |
| translocations | 16 | 3.14% |
| Unknown, only clinical diagn. | 17 | 3.33% |
| Age at 1st consultation (months) | ||
| range | 6-510 | |
| mean ± SD | 71.37 ± 69.71 | |
As we can see in Table 1, the M/F ratio overlaps the same ratio in live born Italian DS babies (Camera e Mastroiacovo, 1984). Even the distribution of chromosomal anomalies fitted the variance range for Italian and International samples.
For these reasons we ought to maintain the present sample as representative at least of the Italian Downs population.
| URTI easiness | No. of Ss | previous surgery * | % |
| not recorded | 6 | 1.46 | |
| not present (0) | 174 | (10) | 33.98 |
| present / mild (1) | 58 | (1) | 11.37 |
| present / moderate (2) | 67 | (5) | 13.14 |
| present / severe (3) | 135 | (3) | 26.47 |
| present / profound (4) | 70 | (2) | 13.58 |
| totals | 510 | (21) | 100.00 |
I found URTI easiness in more than 65% of sample Ss, with greater severity in about 40% of them. In spite of surgical removal of tonsils, adenoids or both this easiness did not disappear in 11 individuals.
In Tables 3-4 I analyzed URTI easiness in infants up to 24 months, and a possible gender influence in infants up to 12 months.
| URTI easiness | No. of Ss | % |
| not recorded | 2 | 1.36 |
| not present (0) | 39 | 26.53 |
| Present, mild (1) | 20 | 13.61 |
| moderate (2) | 22 | 14.97 |
| severe (3) | 40 | 27.21 |
| profound (4) | 24 | 9.72 |
| totals | 147 | 100.00 |
|
URTIeasiness |
No. of F Ss | No of M Ss |
| not recorded | 0 | 1 |
|
not present (0) |
6 | 12 |
| present, mild (1) | 6 | 6 |
|
moderate (2) |
6 | 2 |
| severe (3) | 3 | 8 |
| profound (4) | 4 | 3 |
| totals | 25 | 32 |
Chi Square = 5.187 with 5 df and p = 0.445 NS In first 12 months of life there is not any gender difference to URTI easiness.
| URTI easiness | No. of Ss | % |
| not recorded | 2 | 1.98 |
| not present (0) | 19 | 18.81 |
| present, mild (1) | 8 | 7.92 |
| moderate (2) | 12 | 11.88 |
| severe (3) | 34 | 33.66 |
| profound (4) | 26 | 25.74 |
| totals | 101 | 100.00 |
| URTI easiness | No. of Ss | % |
| not recorded | 1 | 1.35 |
| not present (0) | 17 | 22.97 |
| present, mild (1) | 9 | 12.16 |
| moderate (2) | 8 | 10.81 |
| severe (3) | 29 | 39.19 |
| profound (4) | 4 | 13.52 |
| totals | 74 | 100.00 |
| Urti easiness | No. of Ss | % |
| not present (0) | 14 | 35.90 |
| present, mild (1) | 7 | 17.95 |
| moderate (2) | 4 | 10.26 |
| severe (3) | 11 | 28.20 |
| profound (4) | 3 | 7.69 |
| totals | 39 | 100.00 |
In 73-96 months age interval URTI easiness prevalence is about 65%, and more severe forms run in about 36% of the children.
| Urti easiness | No. of Ss | % |
| not present (0) | 24 | 47.06 |
| present, mild (1) | 2 | 3.92 |
| moderate (2) | 10 | 19.61 |
| severe (3) | 11 | 21.57 |
| profound (4) | 4 | 7.84 |
| totals | 51 | 100.00 |
URTI prevalence in this age interval is about 53% with more severe forms in 29% of the children.
| URTI easiness | No. of Ss | % |
| not present (0) | 23 | 57.50 |
| presente, mild (1) | 4 | 10.00 |
| moderate (2) | 7 | 17.50 |
| severe (3) | 4 | 10.00 |
| profound (4) | 2 | 5.00 |
| totals | 40 | 100.00 |
URTI easiness prevalence in this age interval is about 43% with more severe forms in 15% of children.
| URTI easiness | No. of Ss | % |
| not present (0) | 9 | 56.25 |
| present, mild (1) | 4 | 25.00 |
| moderate (2) | 1 | 6.25 |
| severe (3) | 1 | 6.25 |
| profound (4) | 1 | 6.25 |
| totals | 16 | 100.00 |
URTI easiness prevalence in these 145-168 months old people counts about 44% with more severe forms in 13% of them.
| URTI easiness | No. of Ss | % |
| not present (0) | 14 | 66.67 |
| present, mild (1) | 2 | 9.52 |
| moderate (2) | 2 | 9.52 |
| severe (3) | 3 | 14.29 |
| profound (4) | 0 | 0.00 |
| totals | 21 | 100.00 |
URTI prevalence in this age people goes around 33% with moderate severity in (grade 3) about 14% of them, having the more severe grade four disappeared.
| URTI easiness | No. of Ss | % |
| not recorded | 1 | 4.76 |
| not present (0) | 15 | 71.44 |
| present, mild (1) | 2 | 9.52 |
| moderate (2) | 1 | 4.76 |
| severe (3) | 2 | 9.52 |
| profound (4) | 0 | 0.00 |
| totals | 21 | 100.00 |
URTI easiness prevalence in people aged more than 16 years counts 24% with moderate severity in about 10% of them.
Graphic one shows now the trend of URTI easiness according to age and Graphic 2 the trend of URTI severity according to age.
As we can see, URTI easiness as the sum of four severity grades, decreases in a spontaneous way according to age coming from 80% in years 2-4 to less than 25% after 16. It is to note that 20% of 2-4 years DS children do not catch URTI.
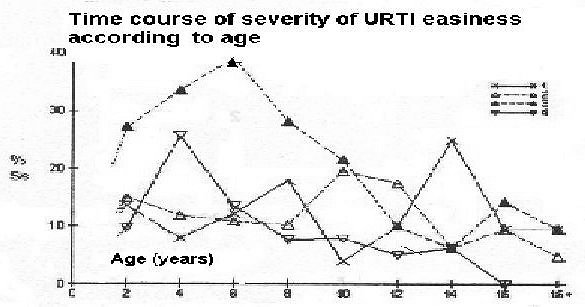
From Graphic 2 we can see that the more severe form (grade 4) goes to a null rate in 14-16 years, while less severe forms do not exceed 10% after this age.
Discussion
This first research is the first step for next research on URTI easiness results in drug treated Down persons. The graduation of the scale used to evaluate URTI easiness is the same I used in previous research (Cocchi, 1987, Cocchi e Bonaduce, 1988; Cocchi, 1990).
The examined sample represents at least the Italian population of 21 trisomics. This is so for its extent, the coming from all Italian regions and the M/F ratio that overlaps what already found in live births of Italian Down children (Camera & Mastroiacovo, 1984).
The distribution of chromosomal diagnoses too, is not far from what usually found either in Italy and foreign countries (Camera e Mastroiacovo, 1984, Hook, 1981).
Fewer subjects with only clinical diagnosis have two explanations. Most of them were adults when they come for 1st consultation, and were born when chromosomal diagnosis did not exist or was not a usual procedure.
Remaining cases refer to babies born in little country hospitals where the clinical evidence was assumed to be enough for the diagnosis. It deals with babies seen only once, and the parents had advice about the need to have a chromosomal diagnosis because the genetic risk of ignoring the presence of a translocation coming out from the balanced translocation of one parent. Since they never came back for checkup, I was unable to update the failing datum, even if the parents had my advice followed.
As for the results, it is immediately to note that the surgical removal of tonsils, adenoids or both did not necessarily make this URTI easiness disappeared. Such surgical removals could have its severity reduced.
In my previous research (Cocchi, 1990) there was a significant gender difference for up to 12 months babies. I supposed it was a bias due to the small sample. By checking it up in this research, it is to exclude a gender influence along with remaining age intervals, already so evaluated in my previous research (Cocchi, 1990).
The use of two graphics to separate URTI easiness from its severity led to observe both parameters in a more exact way. Down persons with more than 16 years have still URTI easiness in about 25% but with a reduced severity by having the grade four disappeared.
Conclusions
The epidemiological research on data I collected during 1st consultations of 510 DS persons allowed to outline the time course of URTI easiness and its severity as a function of age. The 2-4 years' interval represents the more vulnerable age with 80% of sufferers.
The 20% of non sufferers are always a noticeable datum that does not match diffused thinking stereotypes.
Twenty-five percent maintain this URTI easiness among people aged more than 16. Its severity reaches higher rates in infancy but shows a decreasing time course.
This is a preliminary research on drug therapies results on URTI easiness.
References
Camera G., Mastroiacovo P.: Epidemiologia della sindrome di Down. In. Ce.Pi.M. (ed): Aspetti epidemiologici, genetici, clinici, riabilitativi e sociali della sindrome di Down. Ce.Pi.M., Genova 1984: 225-230
Cocchi R. Susceptibility to infective respiratory diseases in depressed children. Epidemiological survey of 126 subjects, clinical-therapeutic report of 61 cases. Acta psychiat. belg. 1981, 81: 350-365.
Cocchi R.: Reduction of susceptibility to upper respiratory tract infections in Down syndrome children following treatment with GABAergic drugs: Report of 70 cases. Int. J. Psychosom. (Philadelphia) 1987, 34/2: 3-7.
Cocchi R.: Facilitá alle malattie infettive respiratorie nei Down. Indagine epidemiologica su 450 casi. Riv. It. Disturbo Intellet. 1990, 3: 131-136.
Cocchi R., Bonaduce D.: Suscettibilitá alle malattie infettive respiratorie in bambini psicotici Down e non-Down. Riv. It. Disurbo Intellet. 1988, 1: 173-178.
Hook E.B.: Down syndrome: Frequency in human popolation and factors pertinent to variation in rates. In: De la Cruz F.F., Gerald P.S. (eds): Trisomy 21 (Down Syndrome) research perspectives. University Park Press, Baltimore, 1981.