Italian Journal of Intellective Impairment 11 (1): 9-17 (1998 Jun)
Via A. Rabbeno, 3
42100 Reggio Emilia, Italy
+39 0522 320 716
Mobile +39 348 5145 520
URL: http://www.stress-cocchi.net
Riverbend DS Assocation Home Page »
» Drug Therapy » URTI Easiness in DSDrug Therapy of Upper Respiratory Tract Infections Easiness in Downs: A Survey on 328 Persons |
Author article list |
|
Renato Cocchi M.D., Ph.D. (Sociology) Italian Journal of Intellective Impairment 11 (1): 9-17 (1998 Jun) |
Reprinted with the permission of Renato Cocchi Via A. Rabbeno, 3 42100 Reggio Emilia, Italy +39 0522 320 716 Mobile +39 348 5145 520 URL: http://www.stress-cocchi.net |
Key words: Down's syndrome; Upper Respiratory Tract Infections; Easiness; Drug therapy.
In my previous research (Cocchi, 1997) I investigated the time-course of easiness to Upper Respiratory Tract Infections (URTI) in 510 non drug treated Downs, as reported at first consultation. Part of them followed drug therapies for different time length, so I can evaluate global therapy results on URTI easiness. The time-course of that easiness will have the comparison with non treated subjects.
Materials and methods
This second survey deals with the clinical records related to all subjects who took the prescribed drug therapy and had at least one checkup after the first visit. This makes a casual consecutive series of Downs that has its selection criterion on the fact that those Downs came back for checkups. As home reared and home living Downs they came from all parts of Italy to outpatients' consultations, between January 1979 and April 1997.
During their 1st consultation all these Ss had their easiness to URTI evaluated and recorded by severity, along with other signs and symptoms. This easiness was appraised with reference to the past 12 months (or, in children aged less than one year, with reference to past months) by recording according to a severity scale as follows:
(0) = as in a healthy child;
(1) = nasal catarrh usually present;
(2) = 1 + susceptibility to cough and cold with few feverish episodes;
(3) = 1 + 2 + easiness to tonsillitis, pharyngitis, bronchitis with moderate fever and limited need of antibiotics (up to four regimens per year);
(4) = 1 + 2 + 3 + high temperatures, occasional otitis and bronchial pneumonia, and frequent use of antibiotics (more than four regimens per year).
I used the same scoring's way during the first checkup or following checkups. From these checkups I collected the scores recorded during the last ones, but some cases came back only once for checkup.
The records about autistic or PDD DS Ss were discarded because we saw that this second heavier pathology can modify the URTI easiness (Cocchi and Bonaduce, 1988).
From the remaining records I collected: sex; chromosomal diagnosis; age at 1st consultation; age at last consultation; length of the drug therapy; scoring of URTI easiness at 1st consultation; the same at last checkup; drugs in use at the last checkup and their daily doses. I processed data by age intervals' statistics and I applied Chi Square Test, when suitable.
Results
Only 328 cards out of 510 fitted the criteria of this survey. They refer to home reared Downs coming from all Italy. Table 1 summarizes epidemiological data of these subjects, table 2 shows drugs in use at last checkups, and tables 3-11 present the URTI easiness scoring according to age intervals.
In graphics 1-5 I showed the time-course of URTI easiness and of each grade of severity, as recorded during the 1st consultation and the last checkup.
| No. of Ss | 328 | 100.00% |
| M | 188 | 57.31% |
| F | 140 | 42.31% |
| M/F ratio | 134.29 | |
| Chromosomal diagnosis | ||
| Standard trisomy 21 | 298 | 90.85% |
| Mosaicisms | 12 | 3.66% |
| Translocations | 12 | 3.66% |
| Unknown, only clinical diag. | 6 | 1.83% |
| Age at 1st consult.: range (months) | 4-410 | |
| Average ± SD |
67.70 ±61.64 |
|
| Age at last checkup: range | 7-417 | |
| Average ± SD |
116.60 ±67.88 |
|
| Length of drug therapy: range | 2-169 | |
| Average ± SD | 48.04 ±43.58 |
| Drug in use | mg/die (*) | no. of Ss | % | ||
| Pyridoxine | 75-150 | 267 | 81.40 | ||
| Diazepam | 1-2.5 | 237 | 72.26 | ||
| S-adenosil-l-methionine | 100 | 190 | 72.26 | ||
| A polyvitaminc compound (BEROCCA)TM | 1 cp x sett | 189 | 57.93 | ||
| L-glutamine | 125-250 | 187 | 45.12 | ||
| Folates | 7.5 | 143 | 43.60 | ||
| Pyritinol | 50-100 | 139 | 42.38 | ||
| Alpha-tocopherole | 50 | 74 | 22.56 | ||
| Vit. B1+B6+B12 | 125+125+500mcg | ||||
| Bromazepam | 0.5-1.5 | 59 | 17.99 | ||
| Biotin | 2.5-5 | 59 | 17.99 | ||
| 5-hydroxytriptofan | 25-50 | 43 | 13.11 | ||
| Arginine pidolas | 250 | 42 | 12.80 | ||
| L-glutamine + pemoline | 45+5 - 90+10 | 41 | 12.50 | ||
| Glycine(in BIOTASSINA)™ | 200 | 34 | 10.37 | ||
| Carnitine | 500 | 34 | 10.37 | ||
| Viloxazine | 50-100 | 22 | 6.71 | ||
| Delorazepam | 0.5 | 18 | 5.59 | ||
| Alpha-ketoglutarato of pyridoxine | 300 | 18 | 4.00 | ||
| Deanol | 320 | 10 | 3.05 | ||
| Oxazepam | 7.5-15 | 9 | 2.74 | ||
| Piracetam | 800 | 7 | 2.13 | ||
| Pantotenate | 150 | 7 | 2.13 | ||
| Amitriptyline+ perphenazine | 10 + 2 | 6 | 1.83 | ||
| Acetyl-carnitine | 250 | 5 | 1.52 | ||
| Clobazam | 10 | 5 | 1.52 | ||
| Taurine | 500 | 3 | 0.91 | ||
| Total | 1802 | ||||
(*) In many cases the drug was prescribed every second day, so the daily dose reports it as it was prescribed every day. The average prescription summed up 5.49 drugs per person. Pyridoxine, alone or in combination with thiamine and cyanocobalamine, and a low dose benzodiazepine were always in it.
| URTI easiness graduation | initial scores | final scores | ||
| No.of Ss | % | No. of Ss | % | |
| Not present (0) | 99 | 30.19 | 221 | 67.37 |
| Present, mild (1) | 37 | 11.28 | 35 | 10.67 |
| moderatea (2) | 49 | 14.94 | 30 | 9.15 |
| severe (3) | 97 | 29.57 | 32 | 9.76 |
| profound (4) | 46 | 14.02 | 10 | 3.05 |
| Totals | 328 | 100.00 | 328 | 100.00 |
| URTI easiness graduation | initial scores | final scores | ||
| No. of Ss | % | No. of Ss | % | |
| Not present (0) | 24 | 24.49 | 10 | 58.83 |
| Present, mild (1) | 14 | 14.28 | 2 | 11.76 |
| moderate (2) | 17 | 17.35 | 1 | 5.88 |
| severe (3) | 26 | 26.53 | 1 | 5.88 |
| profound (4) | 17 | 17.35 | 3 | 17.65 |
| Totals | 98 | 100.00 | 17 | 100.00 |
| URTI easiness graduation | initial scores | final scores | ||
| No.of Ss | % | No.of Ss | % | |
| Not present (0) | 9 | 14.75 | 18 | 40.92 |
| Present, mild (1) | 5 | 8.20 | 6 | 13.63 |
| moderate (2) | 8 | 13.11 | 5 | 11.36 |
| severe(3) | 24 | 39.35 | 12 | 27.27 |
| profound (4) | 15 | 24.59 | 3 | 6.82 |
| Totals | 61 | 100.00 | 44 | 100.00 |
| URTI easiness graduation | initial scores | final scores | ||
| No. of Ss | % | No.of Ss | % | |
| Not present (0) | 8 | 16.33 | 18 | 48.65 |
| Present, mild (1) | 7 | 14.28 | 4 | 10.81 |
| moderate (2) | 4 | 8.16 | 9 | 24.32 |
| severe (3) | 21 | 42.86 | 9 | 24.32 |
| profound (4) | 9 | 18.37 | 3 | 6.11 |
| Totals | 49 | 100.00 | 37 | 100.00 |
| URTI esasiness graduation | initial scores | final scores | ||
| No. of Ss | % | No. of Ss | % | |
| Not present (0) | 10 | 38.45 | 30 | 71.43 |
| Present, mild (1) | 4 | 15.38 | 7 | 16.67 |
| moderate (2) | 3 | 11.54 | 3 | 7.14 |
| severe (3) | 8 | 30.76 | 1 | 2.38 |
| profound (4) | 1 | 3.85 | 1 | 2.38 |
| Totals | 26 | 100.00 | 42 | 100.00 |
| URTI easiness graduation | initial scores | final scores | ||
| No. of Ss | % | No. of Ss | % | |
| Not present (0) | 16 | 43.25 | 28 | 71.80 |
| Present, mild (1) | 1 | 2.70 | 4 | 10.25 |
| moderate (2) | 8 | 21.62 | 4 | 10.25 |
| severe (3) | 9 | 24.32 | 3 | 7.70 |
| profound (4) | 2 | 5.41 | 0 | 0.00 |
| Totals | 26 | 100.00 | 42 | 100.00 |
| URTI easiness graduation | initial scores | final scores | ||
| No. of Ss | % | No.of Ss | % | |
| Not present (0) | 16 | 55.18 | 29 | 72.50 |
| Present, mild (1) | 3 | 10.34 | 6 | 15.00 |
| moderate (2) | 6 | 20.69 | 2 | 5.00 |
| severe (3) | 3 | 10.34 | 3 | 7.50 |
| profound (4) | 1 | 3.45 | 0 | 0.00 |
| Totals | 29 | 100.00 | 40 | 100.00 |
| URTI easiness graduation |
initial scores |
final scores | ||||
| No.of Ss | % | No.of Ss | % | |||
| Not present (0) | 4 | 57.16 | 35 | 79.55 | ||
| Present, mild (1) | 1 | 14.28 | 3 | 6.82 | ||
| moderate (2) | 1 | 14.28 | 1 | 2.27 | ||
| severe (3) | 0 | 0.00 | 5 | 11.36 | ||
| profound (4) | 1 | 14.28 | 0 | 0.00 | ||
| Totals | 7 | 100.00 | 44 | 100.00 | ||
| URTI easiness graduation |
initial scores |
final scores | ||||
| No.of Ss | % | No.of Ss | % | |||
| Not present (0) | 6 | 54.55 | 21 | 80.77 | ||
| Present, mild (1) | 1 | 9.09 | 2 | 7.69 | ||
| moderate (2) | 1 | 9.09 | 1 | 3.85 | ||
| severe (3) | 3 | 27.27 | 2 | 7.69 | ||
| profound (4) | 0 | 0.00 | 0 | 0.00 | ||
| Totals | 11 | 100.00 | 26 | 100.00 | ||
| URTI easines graduation |
initial scores |
final scores | ||||
| No.of Ss | % | No.of Ss | % | |||
| Not present (0) | 6 | 60.00 | 32 | 82.05 | ||
| Present, mild (1) | 1 | 10.00 | 1 | 2.56 | ||
| moderate (2) | 1 | 10.00 | 4 | 10.26 | ||
| severe (3) | 2 | 20.00 | 2 | 5.13 | ||
| profound (4) | 0 | 0.00 | 0 | 0.00 | ||
| Totals | 10 | 100.00 | 39 | 100.00 | ||
In this age group no URTI easiness turned out from 60% to more than 82%, while more severe forms turned down from 20% to a while more than 5%.
Initial and final data as a function of age have summaries in graphic 1 (time-course of no URTI easiness) and in graphics 2-5 (time-course of each grade of severity).
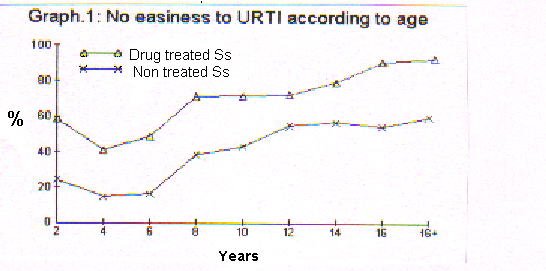
As you can see, drug treated persons have always a higher rate of no URTI easiness.
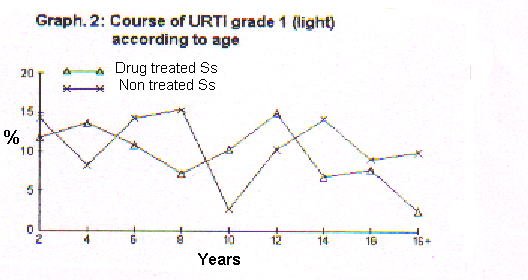
The graphic 2 shows that drug treated subjects have low rates of grade 1 URTI easiness since their 12-14 years of age.
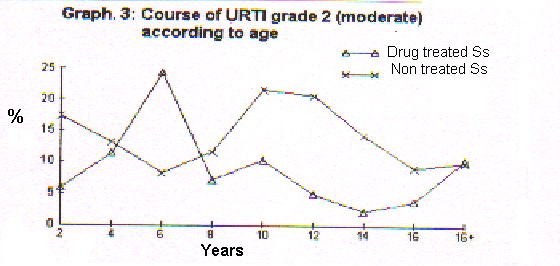
As we can see, since 8 years of age drug treated Downs have a lower rate of grade 2 URTI easiness than non treated Downs. The final peak seems only a statistical artifact.
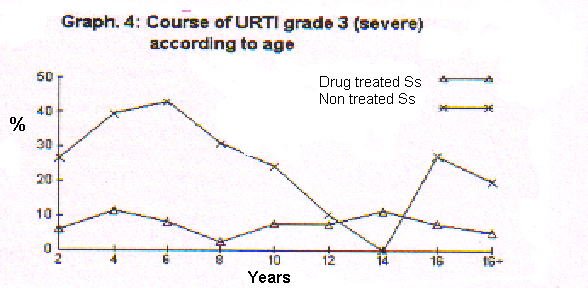
The graphic 4 shows that drug treated Downs had always lesser grade 3 URTI easiness rate than non treated Downs. The null rate in 14 years non treated Downs comes from a statistical artifact.
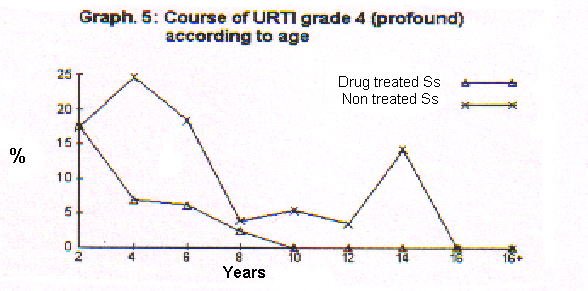
From the graphic 5 it clearly appears that drug treated Downs do not catch the more severe form of URTI easiness since their 10 years. The same fact happens only since 16 years in non treated Downs.
Discussion
This research is the first one on drug therapies for URTI easiness in Down's syndrome that takes into account the age as a favourable factor. The graduation of the scale used for scoring URTI easiness is the same I used in previous research (Cocchi, 1987, Cocchi and Bonaduce, 1988; Cocchi, 1990, Cocchi, 1997). The examined sample represents at least the Italian population of 21 trisomics. This is so for its extent, the coming from all Italy and the M/F ratio overlapping what already found in live births of Italian Downs (Camera and Mastroiacovo, 1984). The distribution of chromosomal diagnoses too, is not far from what usually found either in Italy and foreign countries (Camera and Mastroiacovo, 1984, Hook, 1981). Being present 6 Ss with only a clinical diagnosis, it does not spoil the distribution congruence of sample chromosomal anomalies.
The average drug therapy lasted four years. The drugs in use at last checkups, as reported in Tab. 2, have a basis on a benzodiazepine and pyridoxine as prescribed alone or together with thiamine and cyanocobalamine. I made the choice of drugs according to signs, symptoms and behaviours of each child, considering both age and the length of the therapy up to now. If I collected the therapies prescribed at first consultations, I had a lesser amount of different drugs. So the presence of l-glutamine, alone or in a compound with pemoline, should have been more significant.
The whole sample had double age stratification in two ways, both for URTI easiness at the age of 1st consultation and URTI easiness at the last checkup. Except infants' age up to 24 months, already debatable because the last checkup happened after average 6 months therapy, subjects compared into the same age interval are nearly all different. This double stratification let to cutting off the variable of the age, so pointing out the effects of the therapies.
In this survey we can already note a surely positive effect of drug therapies per se till 10 years of age. This is confirmed by the early disappearance of more severe forms since 8-10 years, a fact noted only since 16 years in non treated Downs (Cocchi, 1997).
How the probands could get out at such a cut off, I send back to my previous papers as for a whole explanation of action mechanisms, with a wide references support (Cocchi, 1981 e 1987). By shortly summarizing, l-glutamine, pyridoxine and the benzodiazepine as antistress drugs reduce the immune suppressive action of the cortisol. On the other hand l-glutamine acts as a sole supplier of a carbon atom for the production of cells' nuclei. This is of value for the leukocytes nuclei that are the basis of the non specific immunity. I always need to remind that this result, again found in Downs, is not peculiar of them. My first clinical research on this topic dealt with 61 depressed children among which I treated my first Down patient (Cocchi, 1981)
Conclusions
This new retrospective study on narrowing down of URTI easiness in drug treated Downs bears out the previous one (Cocchi, 1987). The result does not depend on the favouring variable of age and it is significant, at least till 10 years of age. After this time the favouring effect of age overlaps the effect of drugs, thus avoiding a clear distinction. This comes out according the type of detection of this study, where I thought out the scoring of the last checkup. Since this is an early and quite firm effect, I have to plan a future research where scoring it at a fixed distance from first consultation. Although I reached now positive results, I think that fixed times of 1 and 2 years would offer more information.
References
Camera G., Mastroiacovo P.: Epidemiologia della sindrome di Down. In. Ce.Pi.M. (ed): Aspetti epidemiologici, genetici, clinici, riabilitativi e sociali della sindrome di Down. Ce.Pi.M., Genova 1984: 225-230
Cocchi R. Susceptibility to infective respiratory diseases in depressed children. Epidemiological survey of 126 subjects, clinical-therapeutic report of 61 cases. Acta Psychiat. Belg. 1981, 81: 350-365.
Cocchi R.: Reduction of susceptibility to upper respiratory tract infections in Down syndrome children following treatment with GABAergic drugs: Report of 70 cases. Int. J. Psychosom. (Philadelphia) 1987, 34/2: 3-7.
Cocchi R.: Facilitá alle malattie infettive respiratorie nei Down. Indagine epidemiologica su 450 casi. Riv. It. Disturbo Intellet. 1990, 3: 131-136.
Cocchi R.: Easiness to upper respiratory tract infections: An investigation on 510 Down's syndrome persons. It. J. Intellect. Impair 1997, 10: 143-149
Cocchi R., Bonaduce D.: Suscettibilitá alle malattie infettive respiratorie in bambini psicotici Down e non-Down. Riv. It. Disurbo Intellet. 1988, 1: 173-178.
Hook E.B.: Down syndrome: Frequency in human popolation and factors pertinent to variation in rates. In: De la Cruz F.F., Gerald P.S. (eds): Trisomy 21 (Down Syndrome) research perspectives. University Park Press, Baltimore, 1981.