The Angle Orthodontist Vol. 69, No. 1 1999, pp. 85-8
The Angle Orthodontist
|
Sindoor S. Desai, BDS; Thomas J. Flanagan, DMD The Angle Orthodontist Vol. 69, No. 1 1999, pp. 85-8 |
Reprinted with the permission of Chris Burke The Angle Orthodontist |
Abstract: The skeletal and soft tissue features, aberrations in dental development, and periodontal and caries characteristics of Down syndrome related to orthodontic treatment are discussed. A case report describing the successful orthodontic treatment of a 13-year-old boy with Down syndrome and a severe malocclusion is presented.Key Words: Down syndrome
The extent of mental deficiency in individuals with Down syndrome has often been exaggerated in the literature, and this may have caused orthodontists to shy away from treating these patients. Because of medical advances and an improved educational system, as well as recognition of oral characteristics, individuals with Down syndrome present with improved and promising health and can be incorporated into any orthodontic practice.
Down syndrome is an easily recognized congenital, autosomal anomaly characterized by generalized physical and mental deficiencies. It affects between 1 in 600 and 1 in 1000 live births.1 In 1866 John L. Down published a paper describing some of the characteristics of the syndrome that now bears his name.2 Down syndrome is also known as trisomy #21 because approximately 95% of affected individuals have an extra chromosome #21, making the chromosome count 47 instead of the normal 46. Other chromosomal abnormalities included are translocation (3%) and mosaicism (2%).1,3
Down syndrome patients have a stair- or V-shaped palate with a high arch.4 This is caused by deficient development of the midface, and it affects the length, height, and depth of the palate, but not usually the width.5 Perioral muscles are affected by characteristic muscle hypotonia. This leads to a descending angle of the mouth, elevation of the upper lip, and an everted lower lip with tongue protrusion.4 A small oral cavity with a relatively large tongue leads to mouth breathing, which is a common cause of chronic periodontitis and xerostomia.6 A hypotonic tongue shows characteristic imprints of teeth along the lateral border. A scalloped (crenated) and plicated (scrotal) tongue is also common.7
Platybsia,5 which refers to the obtuse NSBa angle (nasion-sella-ba-sion), leads to a flat cranial base. Because there is simultaneous maxillary deficiency, the mandible is not rotated down and back. Bosma and Dibbets8 found that the morphology of the lower jaw is normal but the symphysis is not. Fisher-Brandies9 concluded that mandibular size is initially normal but becomes mildly hypoplastic by age 14. The gonial angle develops normally. The midface is more deficient than the mandible.5
Kissiling10 reported the following findings in patients with Down syndrome: Mandibular over jet, 69%; anterior open bite, 54%; posterior cross bite, 97%; Class III occlusion, 65%; and maxillary and mandibular incisor protrusion. The freeway space is about three times the normal value of 2 to 3 mm.
Between 35% and 55% of individuals with Down syndrome present with microdontia in both the primary and secondary dentition.10 Clinical crowns are frequently conical, shorter, and smaller than normal, and the roots are shorter as well. Tooth agenesis or defective development is ten times more likely in patients with Down syndrome than in the general population.11 The teeth most affected by agenesis are mandibular central incisors, followed by maxillary lateral incisors, second premolars, and mandibular second premolars. Canines and first molars are rarely affected. The timing of eruption is delayed in both the deciduous and permanent dentition, and the sequence is also affected.12 The central incisors still erupt first and the second molars are usually last but in between, the sequence of eruption varies greatly. Ondarza et al.13 showed a higher frequency of malalignments in both the deciduous and permanent dentition in individuals with Down syndrome.
 |
 |
 |
|
||
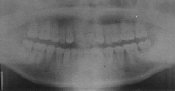
| Pretreatment panoramic radiograph | |||||
Figure 1A |
Figure 1B |
Figure 1C |
|||
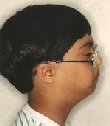
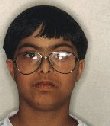
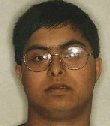
| Pretreatment facial photographs | |||||
 |
 |
 |
Figure 3A |
Figure 3B |
Figure 3C |
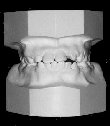
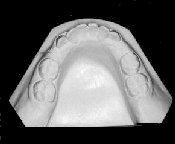
| Pretreatment intraoral photographs | ||
|
|
|||||||||
|
||||||||||
Some individuals may have open-mouth posture leading to abnormal intraoral pressure and oromuscular movements. This causes incoordination of the velum, lips, and cheeks in swallowing and speech.
Individuals with habitual mouth breathing tendencies are more susceptible to periodontal disease, with onset as early as 6 to 15 years. Breakdown is more rapid and generalized in adulthood.14 Implementation of an oral hygiene program should be stressed.
The prevalence of dental caries in patients with Down syndrome is low.14 This is a favorable factor in management of orthodontic patients. The following case report is an example of successful orthodontic treatment of an individual with Down syndrome and a challenging malocclusion.
Patient SD presented at 13 years 1 month, a male Indian with Down syndrome. He was not taking any medications at the time, and his medical history was unremarkable. A panoramic radiograph indicated that the maxillary lateral incisors were congenitally missing and the maxillary canines and first premolars were transposed. The etiology for this malocclusion is believed to be a combination of Down syndrome and heredity.
 |
 |
 |
|
||
| Posttreatment panoramic radiograph | |||||
Figure 6A |
Figure 6B |
Figure 6C |
|||
| Posttreatment facial photographs | |||||
 |
 |
 |
Figure 8A |
Figure 8B |
Figure 8C |
| Posttreatment intraoral photographs | ||
|
|
|||||||||
|
||||||||||
The patient was in the mixed dentition with a Class II malocclusion, congenitally missing maxillary lateral incisors, transposed maxillary canines and first premolars, and with a moderate mandibular arch-length discrepancy. The mandibular deciduous second molars were still present. Mandibular incisor angulation was high, but not unexpectedly so, due to the forward tongue position associated with Down syndrome. There was a 7 mm overjet, and the cephalometric analysis indicated a Class II. skeletal pattern due to the retruded mandible. The maxillary and mandibular incisors were protrusive. The profile was convex, with a lack of a soft tissue chin, and the lips strained at closure.
Treatment was initiated May 1993 with the extraction of the maxillary deciduous canines and the maxillary and mandibular deciduous second molars. Cervical traction was initiated and a mandibular lingual arch was placed until eruption was complete. Extractions were done to enhance vertical eruption of the maxillary first and second premolars and a holding arch was placed to prevent molar migration while awaiting eruption. Full .022 × .025 edgewise appliances were placed April 1996. Elastics were not used. Bands were removed 3 months later and retainers were placed. Total treatment time was 3 years 2 months. Patient compliance was good.
Changes in the maxilla were minimal, with SNA remaining constant at 80°. The maxillary dentition is well aligned, with a moderate reduction in incisor protrusion.
Significant mandibular growth occurred, mainly in the horizontal direction. ANB decreased from 7 to 4 degrees, and the mandibular plane remained unchanged. The mandibular arch was also well aligned and the mandibular incisors upright. Ideally, the incisors would have been uprighted even more; however, due to the forward tongue position associated with Down syndrome, a higher incisor angulation seemed acceptable.
A Class II molar/Class I canine occlusion was achieved, with acceptable overjet and overbite. The facial profile was Class I, with a reduction in facial convexity. The lips were well balanced and the soft tissue contours pleasing.
A maxillary Hawley retainer and mandibular Tru-Tain retainer were placed.
This case study demonstrates that an individual with Down syndrome can be an excellent orthodontic patient and should not be excluded from the patient population. A stable occlusion was achieved along with pleasing soft tissue contours.
Author Address
Dr. Sindoor Desai
P. O. Box 509
Cleveland, NY 13042